Foot & Ankle
MEDICAL TREATMENTS (NON-SURGICAL)
SURGICAL TREATMENT
MEDICAL TREATMENTS (NON-SURGICAL)
The adaptation of footwear with more cushioning and a slight heel is a simple way to reduce pain at the beginning of the symptoms. Medications (pain relievers and anti-inflammatories) prescribed by your primary care physician can help combat acute pain and inflammation.
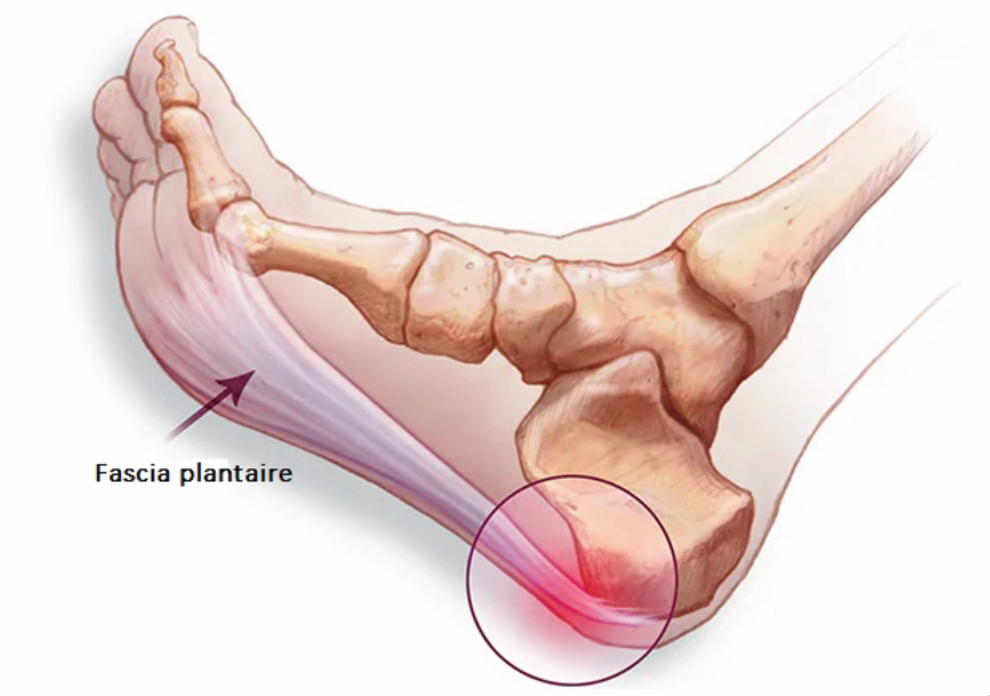
Reducing contributing factors such as rest or weight loss should be the first measures considered. Correcting structural foot problems with the use of orthotic insoles (orthopedic shoe inserts) is an excellent way to relieve inflammation of the plantar fascia.
Rehabilitation physiotherapy, involving stretching of the plantar fascia and the entire suro-achilleo-plantar chain, helps reduce pressure and inflammation. Deep transverse massages can also be performed.
The use of shockwaves, mesotherapy, or local cortisone injections is excellent therapeutic methods to reduce inflammation.
Without treatment, heel pressure becomes increasingly painful, leading to limping with a lack of support and difficulties in wearing shoes.
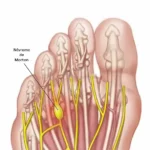
In the worst-case scenario, fibrous nodules can form within the inflamed plantar fascia, and even a rupture of the fascia can occur.

SURGICAL TREATMENT
Important Point: The “ossification” image at the insertion point of the plantar fascia on the heel bone is often misinterpreted by patients as the cause of their pain, resembling a “painful spur” that should be removed.
However, this “bony spur” is not inherently painful; it is merely a reflection of the mechanical tension at the bone insertion of the plantar fascia.
Therefore, treatment involves lengthening the plantar fascia, and the removal of the ossification has no benefit!
When conservative treatment is insufficient, surgical intervention may be proposed. Surgical treatment involves partial or total sectioning of the plantar fascia, which then heals in a relaxed position, reducing pressure within it. Inflammation subsequently resolves on its own.
Sometimes, surgical treatment is part of a more comprehensive approach to correcting structural abnormalities in the midfoot or hindfoot. The procedure on the plantar fascia is just one step in releasing the midfoot or hindfoot.