Hand & Wrist
A pinched nerve :
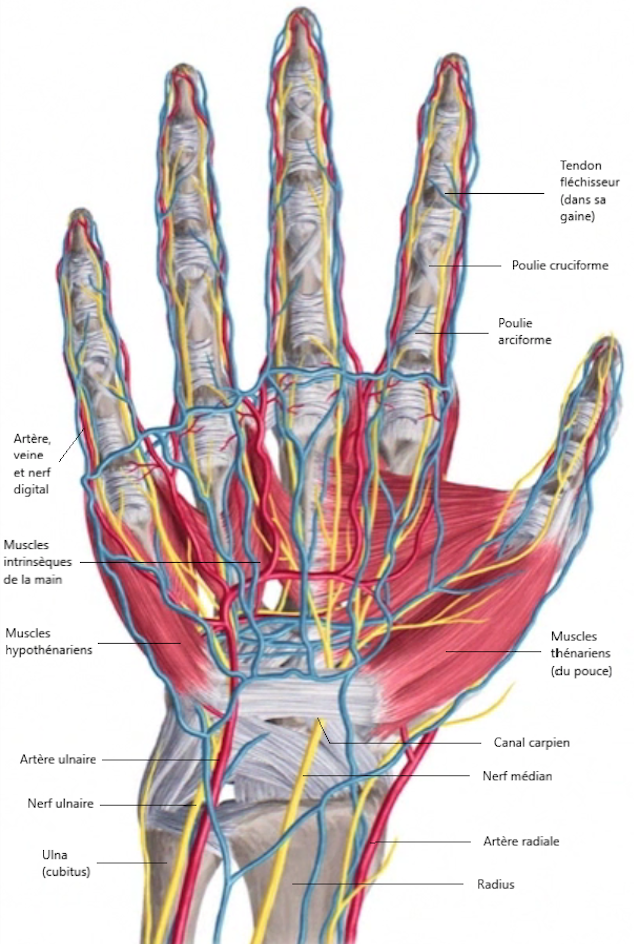
The carpal tunnel is a narrow and non-expandable tunnel located on the anterior side of the wrist. Its walls are formed by the bones of the wrist at the back and sides, and at the front by a thick ligament called the anterior annular ligament of the carpus.
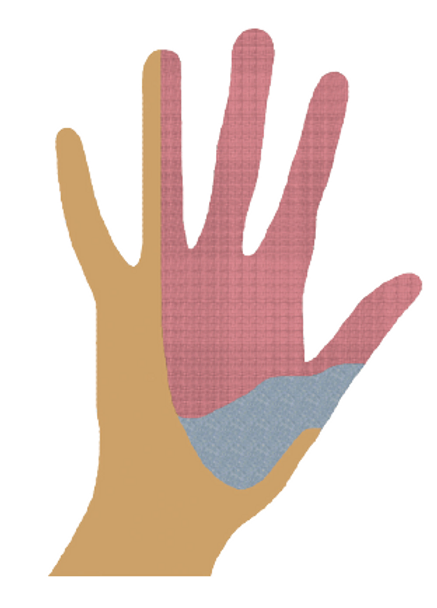
Within this tunnel, the flexor tendons pass, and most importantly, the MEDIAN NERVE, which provides sensation to the fingers (thumb, index, middle, part of the ring finger) as well as some thumb movements.
With age, manual work, repeated external compression (e.g., computer work…), this tunnel narrows, and the nerve becomes compressed. Less commonly, other causes can be identified, such as an increase in the volume of flexor tendons and their sheaths due to certain medical conditions (diabetes, hyperthyroidism, amyloidosis…) or the development of cysts or other masses inside the canal.
Women are more affected than men:
Carpal tunnel syndrome affects women twice as often as men.
It typically appears in women around the age of 50 and in men between the ages of 30 and 50, especially those who have jobs that require repetitive and strenuous wrist movements or the use of vibrating machinery. The frequency and severity of the syndrome increase with age, and it often affects both wrists.
Tingling and burning sensations that wake you up at night :
Unlike other hand conditions (such as arthritis, tendonitis, etc.), the symptoms of carpal tunnel syndrome primarily occur at rest, often during the night.
The patient is awakened by painful tingling, burning sensations, and numbness in the fingers, which they try to alleviate by lowering the hand, shaking it, placing it under water, etc. The pain can radiate up to the shoulder.
Compression of the nerve can also lead to a loss of sensation, dexterity, and motor strength in the fingers in severe cases (primarily in the thumb, index, and middle fingers). The patient may start dropping objects and have difficulty opening a jar, etc.
A clinical examination to rule out other conditions :
In addition to analyzing the patient’s described symptoms, the surgeon performs a clinical examination to confirm the diagnosis of carpal tunnel syndrome. They must also rule out the possibility of nerve compression at the elbow or cervical spine, which can sometimes mimic carpal tunnel symptoms. The surgeon may also prescribe an electromyogram (EMG), an examination conducted by a neurologist.
Furthermore, they investigate underlying conditions (such as diabetes, hyperthyroidism, etc.) and conditions frequently associated with carpal tunnel syndrome, such as trigger finger and Dupuytren’s disease.
The current has difficulty passing through :
The electromyogram (EMG) is a non-irradiating test that confirms a diagnosis of carpal tunnel syndrome and measures its severity. The test involves placing an electrode at the shoulder and another at the fingertips.
The electrode at the shoulder sends a small electrical stimulus, and the electrode at the fingertips records the response. This allows for the calculation of the speed of stimulus conduction and the detection of any slowing of this conduction (at the elbow or wrist for carpal tunnel syndrome).
The treatment :
There are many paramedical treatments (acupuncture, osteopathy, ultrasound, yoga, magnets, etc.), but their effectiveness has not been scientifically proven, just like the night splint. For mild to moderate carpal tunnel syndrome, local infiltration can be effective for a duration ranging from a few days to several months. It can be repeated two or three times in total.
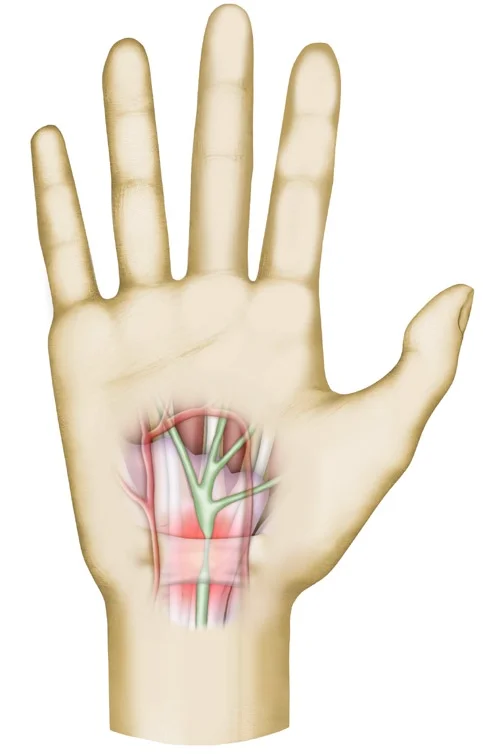
In severe cases, carpal tunnel release surgery is indicated without delay, to prevent incomplete symptom recovery. The operation, which lasts about twenty minutes, aims to widen the diameter of the carpal tunnel by cutting the anterior annular ligament of the wrist. It is performed under local regional anesthesia (only the arm is numbed), on an outpatient basis. It can be done as an “open” procedure with a 1.5cm incision or endoscopically.
Regardless of the surgical approach chosen by the surgeon, the benefit is immediate. The tingling and pain disappear on the same day as the surgery. Sometimes, when carpal tunnel syndrome is very advanced, and especially when it is treated late, complete and normal sensation may only return after a few months or not at all, underscoring the importance of early intervention.
Mild post-operative effects:
Postoperatively, the patient can move their fingers and wrist freely and use their hand for gentle everyday activities (eating, grooming, etc.). Forced or repetitive movements are prohibited for the first eight weeks.
Simple nursing care is required, such as changing the dressing every 2-3 days for two weeks. The surgical incision should not get wet during this period. The average time off work is three weeks and depends on the type of job and the ability to “take it easy” with the operated hand during the first few weeks of resuming work.
An evolving healing process :
The scar evolves over time. Initially soft and thin during the first week, it hardens and thickens before gradually fading in the subsequent weeks. Typically, the scar is fully healed by the end of the second week. Occasionally, there may be slight sensitivity when applying pressure to the palm at the surgical site. This sensation usually disappears within 3 to 6 months following the surgery.
Complications that remain rare :
Infections at the surgical site are exceptionally rare and of low severity if treated promptly. Other complications such as the sectioning of a nerve, tendon, or artery during the procedure are extremely rare.
Sometimes, symptoms may persist, most often due to inadequate release of the ligament. A second surgery is then performed. Recurrence of symptoms (relapse) is exceptionally rare. A consultation with the surgeon is necessary to conduct new examinations to check for possible fibrosis around the median nerve and decide on the appropriate treatment (medical or surgical).
Finally, in rare cases, patients may suffer from complex regional pain syndrome (CRPS), a painful regional syndrome characterized by diffuse stiffness in the entire area beyond the scar, often self-resolving after several months. Its resolution can be accelerated by intensive physiotherapy, coupled with regular follow-up by the surgeon.
Adapted from the information sheet of the SOFCOT (French Society of Orthopedic and Traumatological Surgery).

