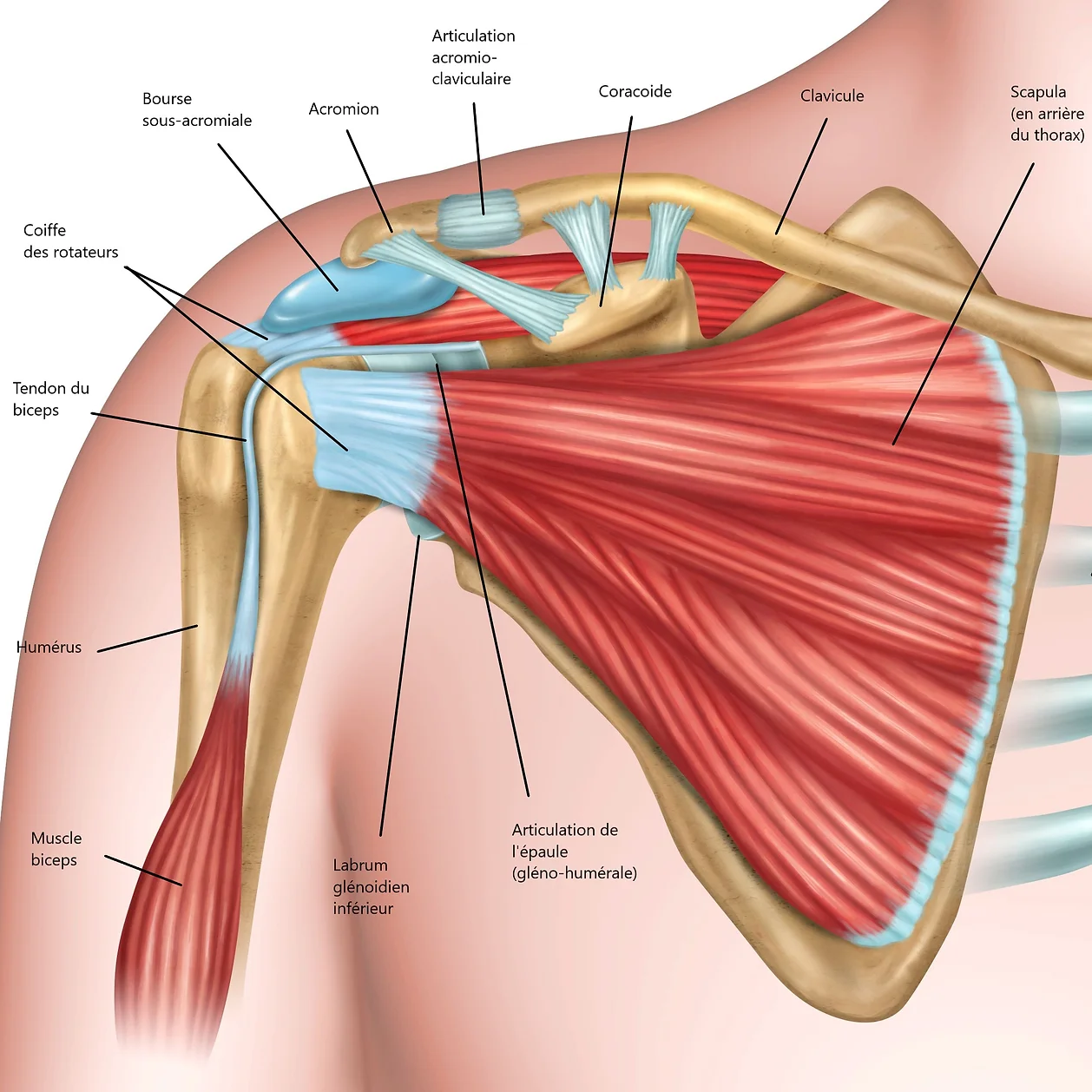
The scapula (shoulder blade) is a flat bone suspended on the posterior side of the ribcage by a large number of muscles.
It has two lateral bony expansions:
The glenoid, covered by a white, hard, and very slippery substance called cartilage.
The acromion, which forms our “shoulder pad,” palpable under the skin. This is where the stars of army officers rest!
The shoulder is a combination of two joints:
Glenohumeral joint
This joint is between the glenoid, a small flat surface about the size of a two-euro coin, and the proximal end of the arm called the humeral head, which is shaped like a large sphere. This joint naturally has an unstable, non-congruent bone structure. It is held in place by ligaments, muscles, and a 5mm elastic joint that surrounds the glenoid, increasing its effective surface area, called the labrum.
The weight of the arm is attached and suspended by all these "soft" structures. However, the incongruent conformation of the glenohumeral joint gives it a major advantage, which is the ability to move in almost all planes, making it the most mobile joint in the human body.
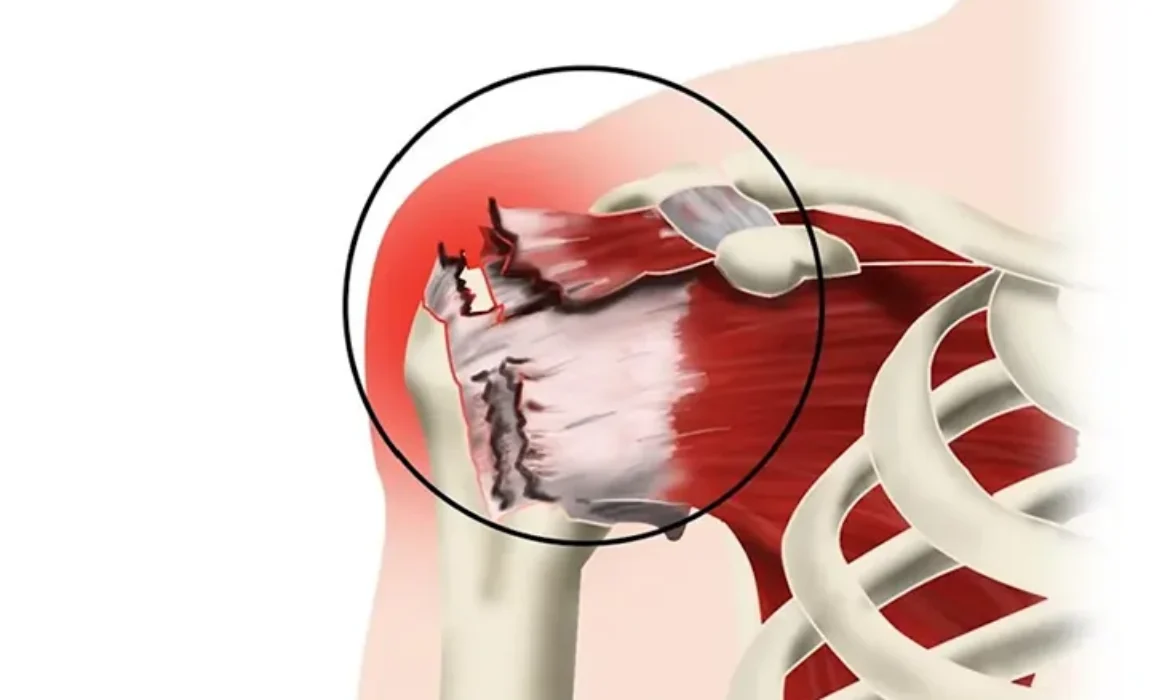
➜ Rotator Cuff Disease: The great mobility of the shoulder is made possible by five tendons that insert themselves around the circumference of the humeral head, resembling a cuff. We will mainly focus on the supraspinatus tendon, which allows lifting the arm to the side and forward, the infraspinatus, which enables external rotation of the arm, and the subscapularis for internal rotation.
With age, and especially with certain professional activities, sports, or repetitive vicious positions, these tendons can become inflamed, causing pain and limited movement. Over time, this can progress to degeneration of the tendon tissue, with the development of fissures and possibly tendon rupture.
Different stages of rotator cuff disease may require a wide range of treatments, ranging from physiotherapy to surgical repair, as well as one or more local infiltrations. Naturally, this should be combined with discontinuing the activities/movements/repetitive vicious positions that caused this condition.
➜ Glenohumeral Arthritis: Like any joint, the glenohumeral joint can also suffer from arthritis, with drying and erosion of the cartilage over time. The bony edges of the joint are exposed and rub against each other with each movement, causing pain.
Shoulder prostheses are a radical and effective solution in these cases, and the choice of prosthesis type (hemiarthroplasty, total prosthesis, reverse prosthesis) is made based on several criteria, including the condition of the rotator cuff. Some comminuted fractures of the humeral head, which cannot be fixed, may also require replacement with a prosthesis.
➜ Glenohumeral Instability: Shoulder dislocation is the complete dislocation of the humeral head, most often forward against the chest, leaving the shoulder socket empty. It is a very violent phenomenon, accompanied by tearing of ligaments, the labrum, and sometimes even tendons and bone fragments. These elements normally act as barriers to keep the head securely in front of the glenoid. After reducing the dislocation, we can hope for healing of these structures with strict immobilization, supplemented by gradual rehabilitation.
In cases where this healing is incomplete or insufficient, dislocation may recur. In such cases, surgical intervention may be necessary, either to tighten the ligaments and reattach the labrum (Bankart procedure) or to screw a bony fragment onto the glenoid, creating a bony stopper (Latarjet procedure).
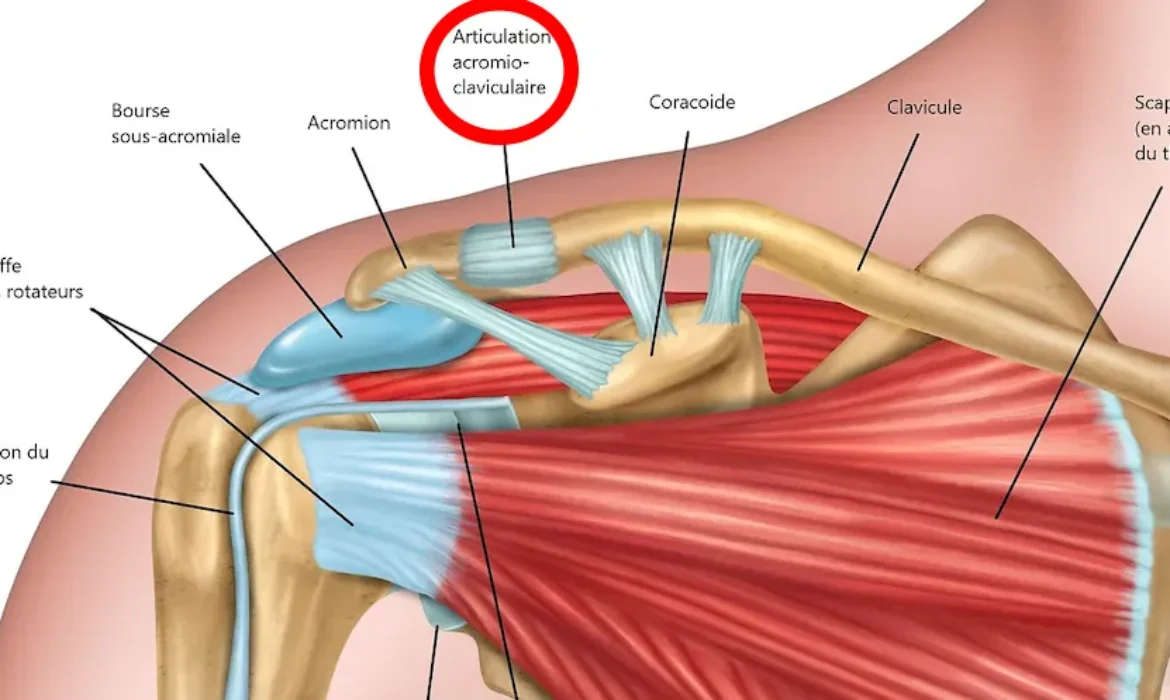
The Acromioclavicular Joint
It is almost immobile and is located between the acromion and the clavicle. It acts like a hanger through which the clavicle "carries" the weight of the arm and the scapula.
A fracture of the clavicle or a dislocation of the acromioclavicular joint causes the entire arm/scapula assembly to "fall," held only by soft tissues.
In mild to moderate cases, such injuries can be treated with well-conducted immobilization, followed by rehabilitation. In severe cases (displaced acromioclavicular fractures or dislocations), it is necessary to realign the "acromioclavicular hanger" and fix it rigidly enough (screwed plate, pinning, ligament reconstruction, etc.).
Shoulder instability is a condition where the upper arm bone (humerus) does not stay properly centered in the shoulder socket (glenoid), leading to a partial or complete dislocation. This can cause...
For proper functioning, the shoulder requires integrity of the bony surfaces as well as good function of the deltoid muscle (which gives the shoulder its contour) and the muscles of the rotator cuff...
THE CONDITION :
The rotator cuff of the shoulder consists of five tendons: the supraspinatus, the infraspinatus, the subscapularis, the long head of the biceps, and the teres minor. Together, these...
It is a small, nearly immobile joint located between the acromion and the clavicle. It acts as a rigid hanger, with which the clavicle “supports” the weight of the arm and the scapula.
A...