Shoulder
THE CONDITION :
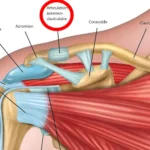
The rotator cuff of the shoulder consists of five tendons: the supraspinatus, the infraspinatus, the subscapularis, the long head of the biceps, and the teres minor. Together, these tendons form a continuous sheet that covers the head of the humerus like a “cuff.” They slide back and forth under the acromion, the bone of the shoulder blade.
The rotator cuff provides the shoulder with a wide range of motion, including forward elevation, abduction, adduction, external rotation, and internal rotation.
With age, and especially with certain occupational activities, sports, or repetitive awkward positions, these tendons can become inflamed and progressively wear out.
Two mechanisms often evolve concurrently:
- Biological degeneration of the tendon tissue itself (intrinsic wear).
- Repetitive mechanical rubbing of the tendons against the edge of the acromion, known as subacromial impingement.
Gradually, micro-tears develop within the tendons (tendinopathy), which can progress over the long term to a partial or complete rupture of the affected tendon. The rupture can occur slowly and progressively or very quickly, spontaneously or after trauma. It is more likely to occur when the tendon is degenerative.
On the other hand, a very violent trauma is required to rupture a healthy tendon, such as in young athletes, for example. In most cases, these situations require prompt surgical repair.
DIAGNOSIS :
The diagnosis of rotator cuff tendinopathy is primarily clinical. Clinical examination helps detect tendon pain or rupture, as well as other possible causes of pain.
The initial imaging tests often performed are X-rays. They can reveal, among other things, small “flakes” of calcium, corresponding to intratendinous calcifications, which indicate tendon degeneration.


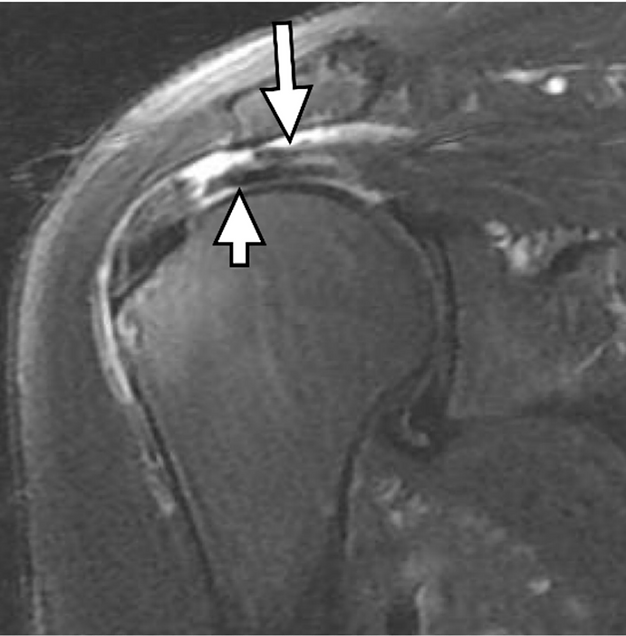
MRI (Magnetic Resonance Imaging) is very effective at visualizing soft tissues, including the tendons of the rotator cuff. Several classifications are used to assess the severity and chronicity of the condition, taking into account the quality of the tendon tissue, the corresponding muscle, joint cartilage, the degree of retraction of a ruptured tendon, and more.
Arthroscopy (scanner preceded by the injection of a contrast agent into the joint) is also a valuable tool that can help us make a more comprehensive diagnosis.
TREATMENT:
Surgical intervention for rotator cuff tendinopathy is not always necessary. Many patients with partial tears can experience functional improvement and reduced pain with well-conducted non-surgical treatment.
Non-surgical treatments, often used concurrently, typically span over several months and require serious commitment from the patient. These non-surgical treatments may include:
- Relative rest for your shoulder to allow the tendon time to heal. This may involve modifying some activities, carefully selecting sports, and avoiding repetitive harmful habits.
- Physical therapy with stretching and selective strengthening of specific shoulder muscles.
- Pain relievers and anti-inflammatory medications (NSAIDs) to minimize pain and inflammation.
- Corticosteroid injections to reduce inflammation and pain.
- Platelet-Rich Plasma (PRP) injections to promote healing.
Surgical Treatment :
Surgical intervention is proposed if you have a large or transfixing tear, or if non-surgical methods are insufficient to heal a partial tear.
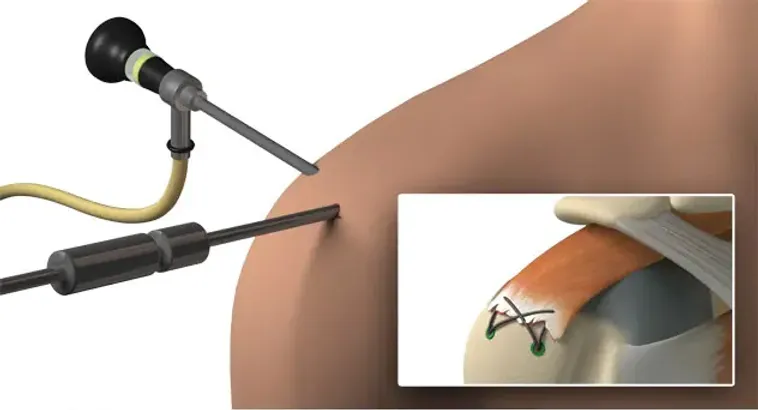
The surgery is most often performed arthroscopically, with 3 or 4 small skin incisions, each approximately 1 cm in size.
In the majority of cases, this is an outpatient surgery. You will return home on the same day with immobilization using a Dujarrier-type sling for 2 to 6 weeks, depending on the case.
Post-operative rehabilitation begins at 2-3 weeks. It starts with passive movements in the first month, followed gradually by gentle active movements.
Most patients regain shoulder function and strength within three to six months after surgery, but full recovery can take up to 12-18 months.

PROGNOSIS AND PREVENTION :
Surgical repair yields very good results in over 75% of cases. Movement precautions and careful selection of types of activity remain essential, even after successful tendon repair.
Just because a tendon has healed well does not mean it cannot be damaged again, especially if repetitive harmful movements are resumed.
WHEN SHOULD I CONSULT ?
You should consult if you experience:
- Chronic pain in the shoulder and arm.
- Pain that worsens at night or interferes with sleep.
- Redness, swelling, or tenderness in the shoulder joint area.
- Motor weakness in the shoulder or arm.