Foot & Ankle



Non-surgical treatment
Surgical Treatment
The surgery
Les suites post-opératoires
Non-surgical treatment
In general, non-painful hallux valgus deformities can be managed with non-surgical treatment.
A significant portion of mild deformities and discomfort can be successfully managed with proper shoe adjustments.
Your surgeon will provide you with information on proper shoe fit and the type of footwear that would suit you best.
Custom-made orthopedic insoles, protective silicone pads, and toe spacers worn inside your shoe can help cushion the painful area over the bunion.
The effectiveness of orthopedic insoles and small orthoses at this stage is variable, and very few high-quality scientific studies demonstrate their beneficial effects.
Common pain relievers and anti-inflammatories can also help alleviate mild and occasional pain. The consumption of large quantities of pain relievers often indicates the need for an alternative solution.

Surgical Treatment
Surgical correction is considered when pain persists while wearing shoes and walking despite medical treatment.
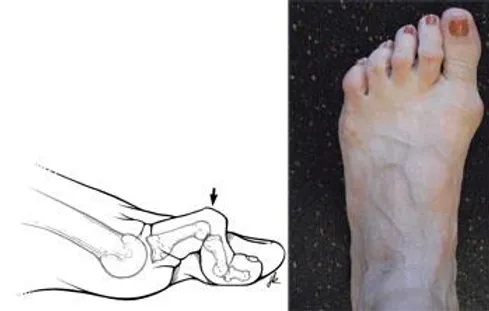
The goal of hallux valgus surgery is to relieve pain by realigning the bone, ligaments, tendons, and nerves so that the big toe can be returned to its correct position and its function in walking propulsion.
Aesthetic reasons alone are not sufficient to justify the intervention.
The surgery
In general, the common goals of most bunion surgeries include:
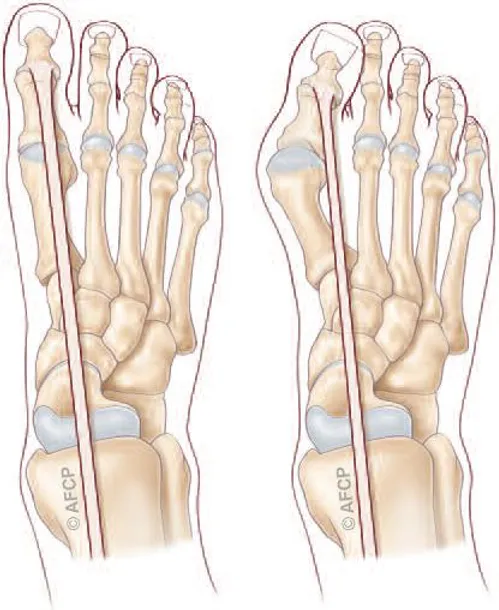
- Realignment of the metatarsophalangeal joint (MTP) at the base of the big toe
- Relieving pain
- Correcting the deformity of the bones that make up the toe and foot
Surgery may involve shortening loose tissues and lengthening tight tissues. This is rarely done without some type of bone realignment, called an osteotomy. In the majority of cases, correction of soft tissues is just one part of the overall bunion corrective procedure.
In an osteotomy, your doctor makes small cuts in the bones to realign the joint. After cutting the bone, your doctor repairs this new break with pins, screws, or plates. The bones are now straighter, and the joint is balanced.
Osteotomies can be performed at different locations along the bone to correct the deformity. In some cases, in addition to cutting the bone, a small wedge of bone is removed to provide enough correction to straighten the toe.
As discussed above, osteotomies are typically performed in combination with soft tissue procedures, as both are often necessary to maintain the alignment of the big toe.
Les suites post-opératoires
Physiothérapie et exercice
Des exercices spécifiques aideront à restaurer la force et l’amplitude de mouvement de votre pied après la chirurgie. Votre médecin ou physiothérapeute peut recommander des exercices utilisant une bande chirurgicale pour renforcer votre cheville ou en utilisant des billes pour rétablir le mouvement de vos orteils.
Des exercices spécifiques tels que l’exercice de ramassage de billes aideront à restaurer le mouvement complet de votre pied.
Commencez toujours ces exercices lentement et suivez les instructions de votre médecin ou de votre physiothérapeute concernant les répétitions.



