Foot & Ankle
ANATOMY :
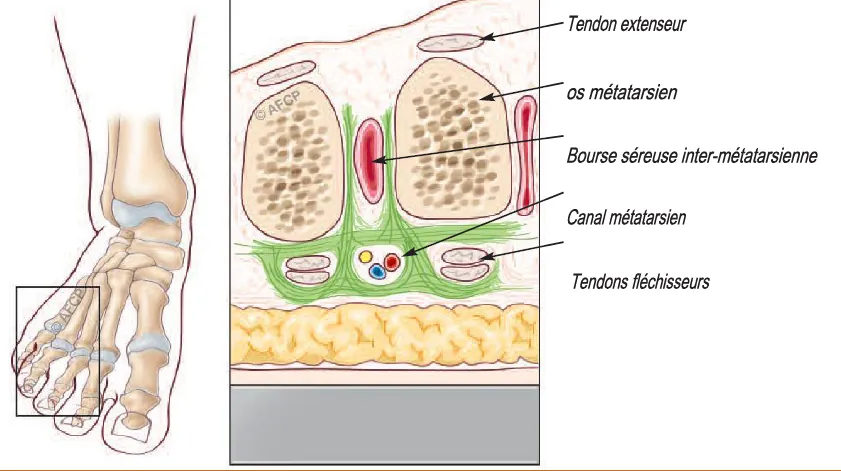
At the level of the toes, sensitivity is ensured by the plantar interdigital nerves, whose division branches ensure the sensitivity of the interdigital commissure. Just before their division, at the level of the space between the metatarsal heads, these nerves pass through a fibrous tunnel called the “metatarsal canal.” The walls of this tunnel are formed: at the bottom by the superficial transverse ligament, at the top by the intermetatarsal transverse ligament, and laterally by fibrous septa connecting these two ligaments. Just above the intermetatarsal canal is a space limited laterally by the metatarsals (bones of the forefoot) containing the tendons of the lumbrical and interosseous muscles and a synovial bursa.
PATHOLOGY :
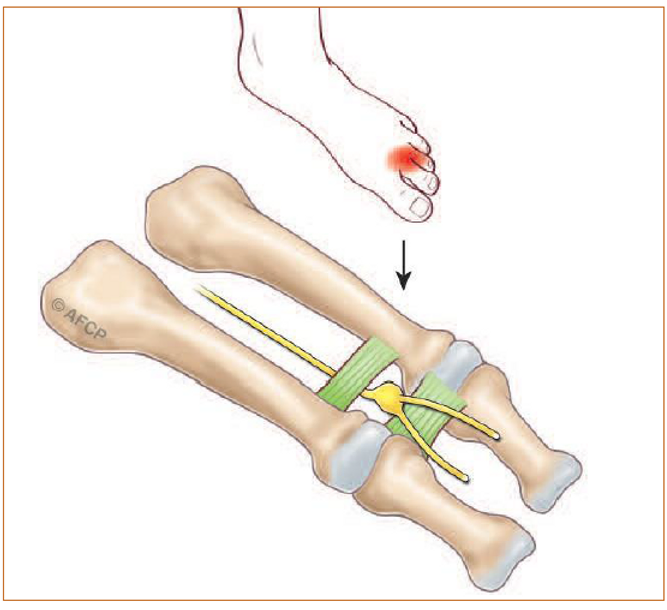
During walking, at the moment of foot impulses on the ground, the nerve is repetitively compressed within the metatarsal canal. This compression can be exacerbated by narrow footwear. This results in nerve irritation.
CLINICAL FEATURES :
Most often, this nerve compression manifests as the onset of severe pain beneath and between the toes.
These pains are often experienced as electric shocks, they may radiate towards the tips of the toes or up towards the ankle. They are generally triggered by walking or prolonged standing, especially if you wear tight shoes.
During a painful episode, removing your shoes and massaging your foot can help alleviate the pain. A tingling sensation or a decrease in sensitivity between the toes is also possible.
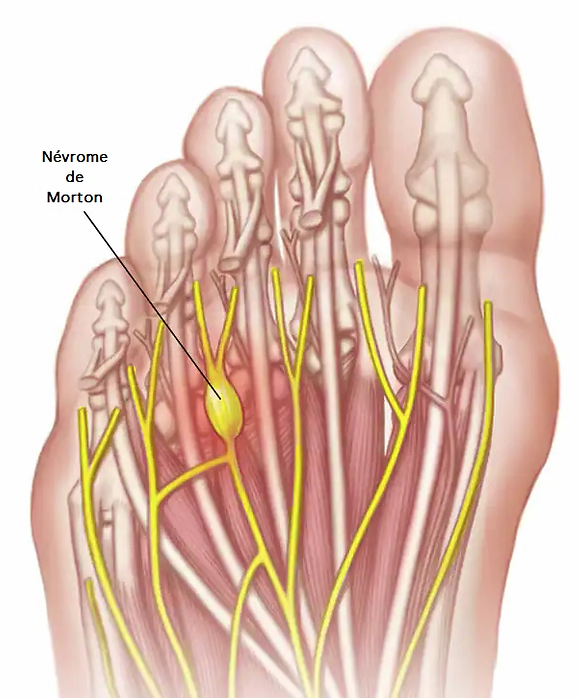
It is possible to have multiple Morton’s neuromas on the same foot or to have concurrent involvement of both feet.
DIAGNOSIS :
During your examination, your surgeon will seek to locate your pain. They will also use specific tests to pinpoint the Morton’s neuroma(s). They may also look for a decrease in sensitivity between the toes.
An ultrasound or MRI may be ordered by your physician or surgeon to visualize the swelling of the nerve or its compression by a neighboring structure. X-rays of the foot are frequently performed to rule out other bone or joint pathologies.
These examinations can also be used to search for pathologies often associated with Morton’s neuroma or to distinguish it from other diseases with similar clinical signs.
TREATMENT OPTIONS :
Firstly, it is recommended to adjust your footwear by wearing shoes with a wide toe box that do not compress the front of the foot and to avoid high-heeled shoes.
Orthopedic insoles (made by a podiatrist) to be worn systematically in your shoes and tailored to your morphology may be prescribed. Their purpose is to reduce repeated pressure on the nerve and thus decrease its irritation.
One or more corticosteroid injections may be administered to decrease or eliminate signs of the condition. When the injection is effective, the relief obtained may be temporary or permanent.
Unfortunately, these treatments do not always control the pain associated with the condition and may be ineffective for some patients. Your surgeon may then suggest surgical treatment aimed at either freeing the intermetatarsal nerve (“neurolysis”) or removing it (“neurectomy”).
In cases where no treatment is undertaken, the pain tends to worsen, resulting in increasingly significant discomfort during walking and wearing shoes.
HOSPITALIZATION :
Your hospitalization can be outpatient (a day hospitalization) or last for a few days depending on your associated conditions, as well as your medical and social situation.
ANESTHESIA :
A preoperative consultation with an anesthesiologist is mandatory. During this consultation, the anesthesiologist will explain the modalities and possible choices of anesthesia tailored to the surgery and your health issues.
During this consultation, your current medication regimen will also be reviewed. New medications may be initiated, either before or after the surgery. The most commonly used ones include anticoagulants, antibiotics, analgesics, anti-inflammatories, etc. They naturally carry specific risks.
The operative anesthesia may be locoregional (wider anesthesia encompassing a segment of the limb, from the leg to the toes), spinal (anesthesia of the pelvis and limbs by puncturing between two vertebrae), or general anesthesia.
Blood transfusion is rare in this type of surgery where bleeding is very limited.
SURGERIES :
During the procedure, your surgeon may encounter an unexpected or unusual situation or event necessitating additional or different actions from those initially planned. Once awake and the surgery is completed, your surgeon will explain the course of action and the procedures performed to you.
Neurolysis involves surgically decompressing the nerve. The procedure typically takes place with the patient lying on their back, a pneumatic tourniquet positioned on the ankle, leg, or even thigh, depending on the type of anesthesia used. The location and size of the scar vary depending on your condition, work habits, and the technique chosen by your surgeon. Usually, the scar is approximately 4 to 5 cm in length. This decompression can be performed through a dorsal incision.
The principle of this intervention is to surgically remove the nerve responsible for the pain. During the surgical procedure, you will be positioned on your back, and a pneumatic tourniquet will be used (positioned on the ankle, leg, or even thigh, depending on the type of anesthesia used). Again, the location and size of the scar vary depending on your condition, work habits, and the technique chosen by your surgeon. It can be performed through a scar located on the top of the foot (Diagram 1), on the sole of the foot (Diagram 3), or in the interdigital commissure (Diagram 2). This intervention frequently results in anesthesia (loss of sensation) or a decrease in sensitivity in the space between the affected toes. For example, during the removal of a neuroma located between the 2nd and 3rd toes, the altered sensitivity will affect the outer aspect of the 2nd toe and the inner aspect of the 3rd toe.
During your time in the operating room, do not be surprised if you are asked multiple times for your identity, the side to be operated on (upon your arrival, during your preparation): this is a mandatory procedure for all patients (referred to as “safety checklist”) and mandated by the Health Authority (HAS).
POSTOPERATIVE CARE :
Specific postoperative footwear is often prescribed according to your surgeon’s protocol.
The dressing is carefully applied during the surgery according to your surgeon’s habits and is usually not to be changed. However, if home care is provided, it is important to ensure the hygiene of your incision as long as the stitches are in place and it is not completely sealed.
Hand hygiene is crucial, and one should never touch the incision without washing hands. Always ensure that you have hand washing facilities or a bottle of hand sanitizer at home for the nurse who will perform your care. On average, care is scheduled for a duration of 15 days to one month.
Prevention of blood clots: The prescription of anticoagulant injections is sometimes considered based on the assessment of your health condition by the surgeon and the anesthesiologist.
Postoperative pain management for this type of condition generally poses few difficulties. Even though strong painkillers may be used immediately after surgery, returning home with simple painkillers is the norm.
Postoperative swelling (swelling of the foot and toes) is common in ankle and/or foot surgery and is usually not a complication. Managing swelling is essential not only to alleviate pain but also to improve the quality of healing. Thus, a certain period of rest, elevation, and the use of compression stockings or varicose vein stockings can be helpful. This swelling can last a long time (several weeks to several months) and usually does not cause any problems, although it may require temporarily adapting footwear.
A period of leave from work is generally necessary after surgery. Its duration is on average one month but depends on your professional activity and the surgical procedures performed.
Postoperative follow-up consultations: Your surgeon will conduct regular clinical, radiological, and biological checks, and the results will be incorporated into your medical record.
The (anonymous) data from your record may be used for studies and/or scientific communications or publications by your surgeon, in compliance with the JARDE law of March 2012 (Decree 2016-1537). In this case, specific consent will be requested by your surgeon and included in your record. Initial consultations focus on monitoring healing and local condition. Subsequent consultations involve monitoring the progress of the procedures performed and your functional recovery.
The implementation of possible functional rehabilitation and the validation of the return to work and sports will be done according to your surgeon’s protocol.
AFTER THE INTERVENTION ?
The aim of the surgery proposed by your surgeon is to alleviate or ideally eliminate the pain associated with Morton’s neuroma.
RISKS :
A surgical procedure is NEVER a trivial matter. Regardless of the precautions taken, there is no such thing as “zero risk.” When you decide to undergo surgery, you must be aware of this and weigh the risks against the expected benefits of the procedure (= benefit/risk balance).
Despite the skills of your surgeon and the team caring for you, unfortunately, every treatment carries a risk of failure. This failure can range from the reappearance of symptoms to their worsening or other more significant risks. These risks may be due to chance, bad luck, but may also be exacerbated by health issues specific to you (known or unknown, local or general).
It is impossible to present here all possible complications, but we have listed below the most common or serious complications that may sometimes occur in your condition.
SENSATION LOSS
SCAR NEUROMA
PERSISTENCE OF SYMPTOMS
CHRONIC PAIN
INFECTION
SENSATION LOSS
After neurectomies, loss of sensation or decreased sensation in the interdigital spaces of the affected toes is common and normal because the sensory nerve has been completely surgically removed. This anesthesia can be total or partial. After neurolysis, the nerve may be traumatized, leading to a decrease in sensitivity or tingling in the interdigital commissure as a result.
SCAR NEUROMA
After a neurectomy, in rare cases, the stump of the severed nerve can heal pathologically (scar neuroma), leading to new pain sometimes requiring a second operation.
PERSISTENCE OF SYMPTOMS
Despite careful nerve release (neurolysis), the neuroma may persist, remain painful, sometimes requiring further surgical intervention.
CHRONIC PAIN
In cases where Morton’s neuroma is associated with other bone or joint pathologies, the clinical outcome of isolated management of the neuroma may be incomplete.
INFECTION
Despite all precautions for disinfection and skin preparation, any surgical incision carries a risk of microbial contamination, which can lead to an infection. These infections can occur early or much later. They often require antibiotic treatment, may necessitate further surgical interventions, and can lead to painful or functional sequelae. Certain factors such as diabetes, smoking, or immunosuppression (corticosteroids, etc.) may predispose to this complication.
RESIDUAL PAIN DUE TO OTHER FOREFOOT PATHOLOGIES :
In cases where Morton’s neuroma is associated with other bone or joint pathologies, the clinical outcome of isolated management of the neuroma may be incomplete.
SCARRING ISSUES
Despite all the care provided by your surgeon to the surgical wound and nursing care, there may be healing disturbances, sometimes exacerbated by a general or local pathology such as diabetes or circulatory insufficiencies, for example. This can result in delayed or impaired healing ranging from an unsightly scar to wound dehiscence or skin necrosis. These scarring issues can also predispose to infection.
THROMBOEMBOLIC COMPLICATIONS
NEIGHBORING COMPLICATIONS
THROMBOEMBOLIC COMPLICATIONS
Any surgical intervention, especially of the lower limb, can predispose to the formation of a blood clot obstructing the veins and causing a thrombosis. This clot can even reach the pulmonary circulation and cause an embolism with sometimes serious or fatal consequences. Prevention of this complication can be achieved by implementing anticoagulation based on the type of surgery and your health condition.
NEIGHBORING COMPLICATIONS
Given the proximity of the surgical area to osseous, tendinous, vascular, or nervous structures, there may be, directly or indirectly related to the intervention, consequences on these nearby elements: hemorrhage, hematoma, paresis, paralysis, numbness, mobility deficit, joint stiffness, etc. Due to the location of the scar, damage to a small nerve can result in numbness or even persistent pain. In some cases, it may be necessary to re-intervene to drain a hematoma, decompress a nerve, release tendons, etc.

