Tibial or femoralosteotomy at the knee is a so-called “conservative” surgical technique used in the treatment of early to moderate knee osteoarthritis, in contrast to non-conservative techniques such as knee prostheses.
Internal knee osteoarthritis is favored by an anomaly in the axis of the lower limb (genu varum, like “Lucky Luke”). When there is an axis defect, the stresses are poorly distributed, and the body weight applies more on the inside, accelerating wear.
Conversely, X-shaped knees (genu valgum) promote wear on the external compartment of the knee. When the osteoarthritis is not too severe yet, it is possible to propose to slow down or even stop its progression by straightening the osseous axis of the knee. The diagnosis of osteoarthritis is confirmed by clinical examination, radiography, MRI, and sometimes arthroscopy.
The mechanical axis of the limb is measured to determine the exact angle of correction needed.
THE SURGERY:
The surgery is performed under general anesthesia or spinal anesthesia, depending on your preferences and especially your medical history.
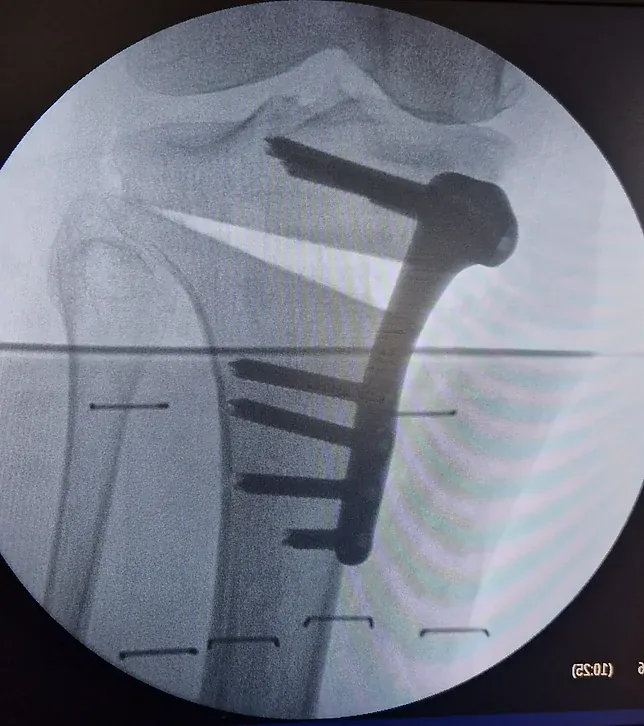
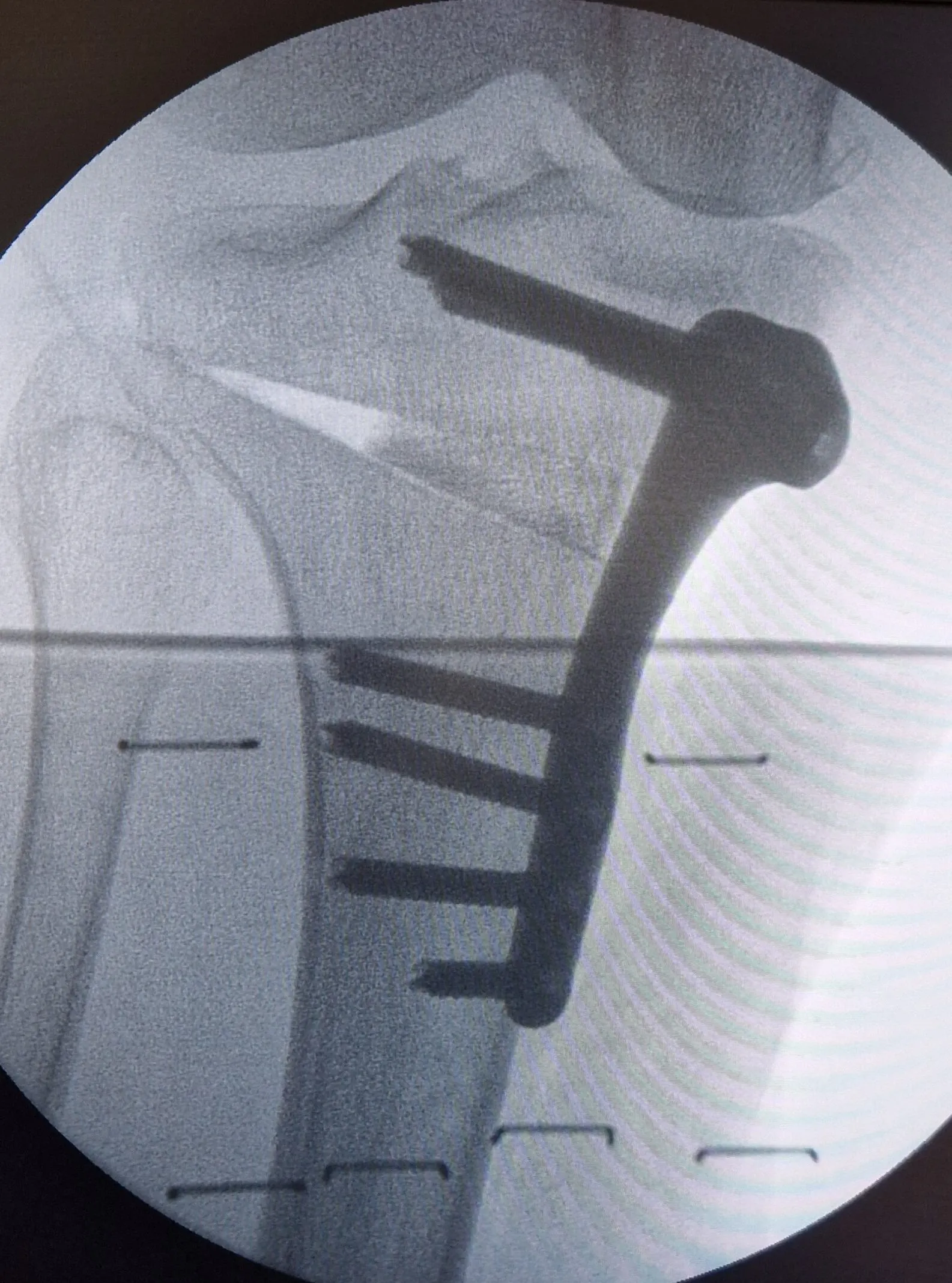
The scar is vertical and averages 8cm in length. A partial cut is made in the bone (osteotomy). An instrument gently spreads the bone edges by a few millimeters, according to the planned correction (8 to 12mm at maximum).
A wedge made of bone graft is inserted into the created space, and a titanium plate that conforms to the anatomical shape of the bone is used to secure the correction.
The surgery is generally performed on an outpatient basis. A physiotherapist comes to see you before discharge to get you standing and to give you practical advice on using crutches. Weight-bearing on the operated limb is prohibited for 6 weeks, the time needed for the osteotomy to consolidate.
During this time, you will be able to move around with crutches, and you will need to have regular sessions (with a physiotherapist and at home) of knee mobilization in flexion/extension, to maintain joint flexibility and prevent muscle atrophy.
An anticoagulant treatment will also be prescribed for 6 weeks.
The consolidation of the osteotomy will be monitored in consultation with regular radiographs. Driving is possible as soon as full weight-bearing is resumed.
EXPECTED RESULTS:
It is very important to understand clearly that a knee osteotomy does not repair the osteoarthritis that already exists in your knee.
Its purpose is to modify a predisposing factor to osteoarthritis, the poor anatomical alignment, in order to preserve what healthy cartilage you have left.
It involves an extra-articular bone procedure, meaning that your surgeon does not touch the inside of your joint.
As a result, you will probably continue to experience the pains associated with osteoarthritis after the osteotomy, sometimes for more than a year, but these will gradually decrease since the pressure on the arthritic compartment is now reduced.
It is therefore appropriate to act seriously and effectively on all the other predisposing factors to osteoarthritis: Excess weight, demanding activities and sports, lifting heavy objects, sedentary lifestyle, etc.
Patient with severe genu varum (Lucky Luke knees, O-shaped) Photo after valgus tibial osteotomy on the left leg
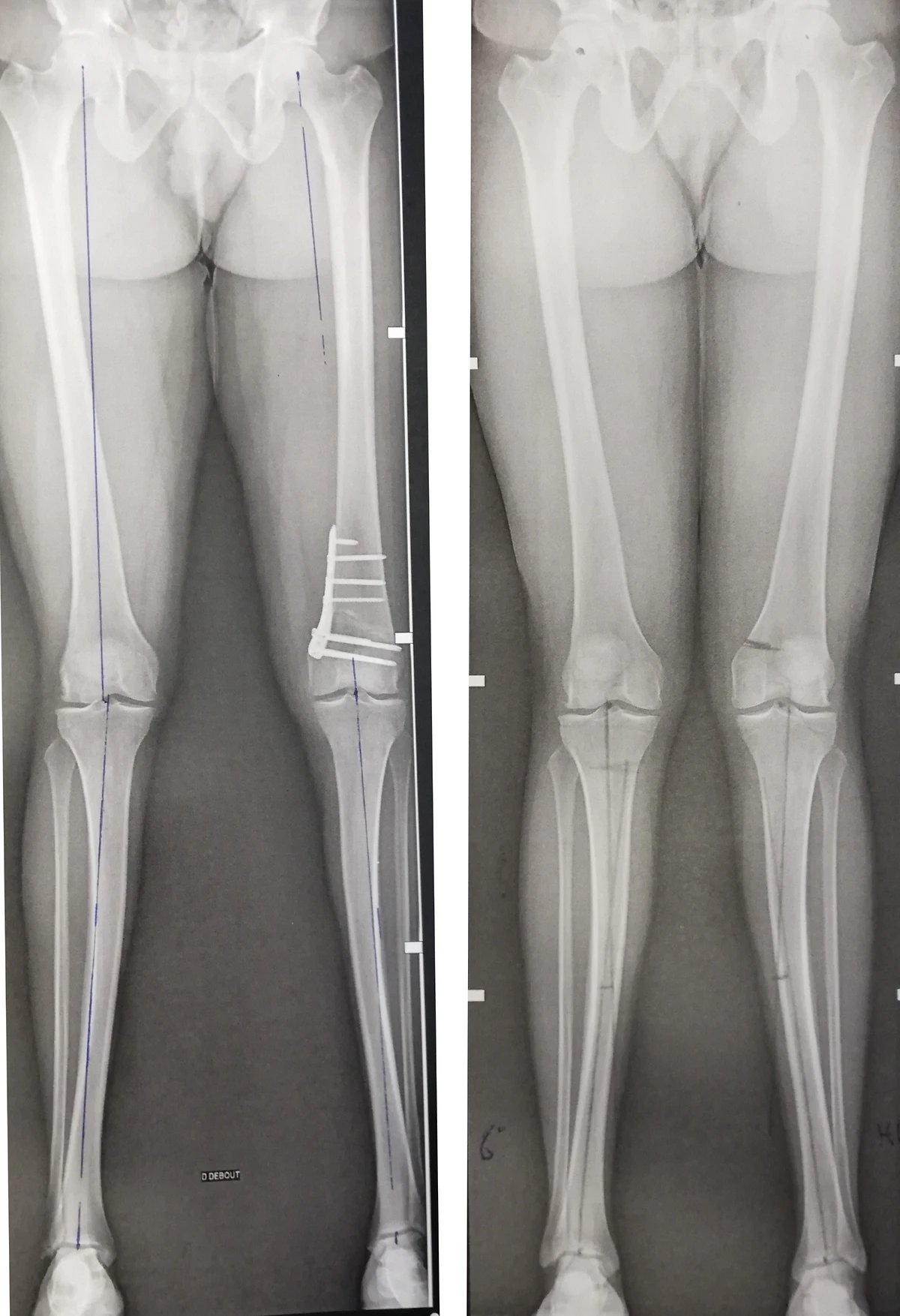
Patient with severe genu valgum (X-shaped knees) X-ray before and after varus osteotomy on the distal left femur. The global mechanical axis of the lower left limb is straight.