Knee
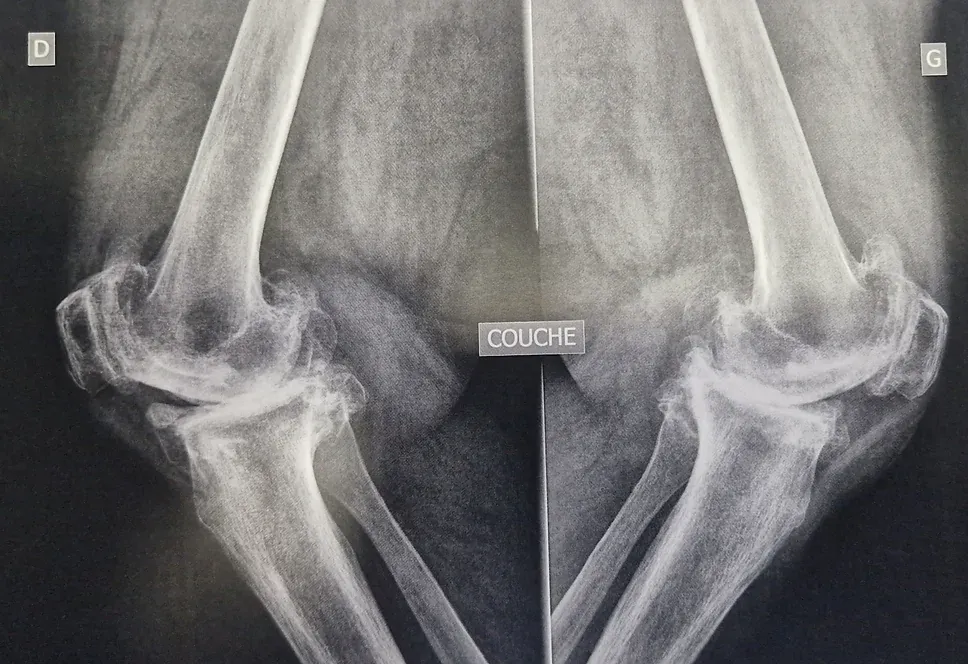
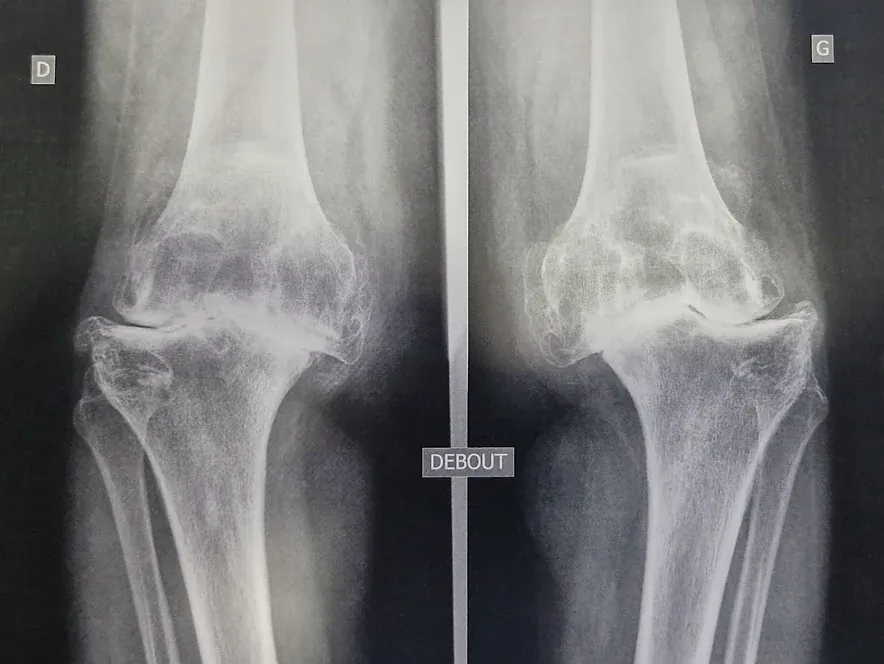
Knee osteoarthritis is a common disease affecting more than one in four people after the age of 65. It leads to a progressive destruction of the knee’s articular cartilage.
The wear of the cartilage is accompanied by a degradation of the menisci, muscles, and synovial inflammation.
It is a global affliction of the joint that becomes painful and starts to stiffen. In some cases, it is no longer possible to fully extend the knee (flexum).
Among the predisposing factors, we can notably mention:
- A misalignment of the knees: “Lucky Luke” knees (genu varum) or X-shaped knees (genu valgum).
- Genetic factor.
- Sequels of old traumas to the bones, cartilage, menisci, or ligaments.
- Overweight.
- The practice of intensive sports or very physical professional activity.
- Inflammatory rheumatism can lead to the destruction of the knee cartilage.
The progression of osteoarthritic disease generally occurs through flares of pain and effusions, lasting a few days to a few weeks, separated by periods of calm of varying lengths.
WHAT ARE THE OPTIONS?
There is no medical treatment available to date that can prevent osteoarthritis or regenerate eroded cartilage. That said, the body often adapts in quite a surprising way to joint wear, sometimes for long durations.
The progression of osteoarthritis can be slowed down by avoiding sports and activities that mechanically stress the knee, and by reducing overweight.
Physiotherapy sessions focusing on muscle strengthening, injections of corticosteroids, hyaluronic acid, or PRP (Platelet-Rich Plasma) can be very beneficial.
These medical measures, when well conducted, can spare the patient from surgery.
But if the pain starts to heavily affect the patient’s daily life and becomes difficult to control with non-surgical means, the surgical option of knee replacement is discussed: It involves freshening the damaged joint surfaces, and “dressing” them with prosthetic parts, thus avoiding painful bone friction.
Contrary to a widely held misconception among the general population, there is no massive bone resection with knee replacement. It is a matter of dressing or “resurfacing” the two damaged joint edges, while preserving as much as possible the other native anatomical structures.
In some cases, the wear is significant but localized to a single compartment of the knee. In such cases, only that compartment can be resurfaced with a partial prosthesis (unicompartmental).
THE SURGERY:
A radiographic assessment is systematically prescribed for you, in order to plan the ideal sizes and positions of the prosthetic implants and to replicate the alignment of the native knee.
Sometimes a CT scan or an MRI is requested to look for a rotational abnormality of the limb or to allow for the manufacture of custom tools specific to your knee, or even to make a tailor-made prosthesis.
A blood test, a urine exam, a cardiology consultation, and a dental assessment are necessary for the medical preparation for the surgery.
The surgery can be performed under general anesthesia or spinal anesthesia, depending on your preferences and especially your medical history. You will be able to discuss this in detail with the anesthetist during the anesthesia consultation.
The surgery generally lasts between 1 to 1.5 hours.
The prosthesis consists of a femoral piece and a tibial piece made of a Chrome-Cobalt alloy, each a few millimeters thick, replicating the native anatomy of the knee. They are fixed to the bone with a medical cement (rapid-setting resin). A polyethylene piece (a very resistant polymer) is placed between the femur and the tibia, ensuring smooth mobility.
At the end of the surgery, a rather thick and slightly compressive dressing is applied. A drain is sometimes used to prevent the formation of a hematoma in the joint. You will stay in the recovery room for an average of two or three hours, where cold packs will be applied to the knee.
A control radiography is performed, then you are taken back to your room. A meal will be served to you there.
POSTOPERATIVE FOLLOW-UP:
Hospitalization after knee replacement surgery generally lasts 3 to 4 nights.
From the next morning, a physiotherapist comes to see you to start mobilizing the knee in flexion/extension, and to have you walk with the aid of a walker or crutches. The physiotherapist will even try to have you climb up and down a few steps before you leave.
The nurses change the dressing every 2 days, which will now be a very thin adhesive dressing. It must remain perfectly clean and dry until the wound is completely healed (2 to 3 weeks). A daily anticoagulant injection is essential to ward off the risk of thrombosis.
You will be able to cover increasingly longer distances. You can dispense with the crutches as soon as you feel stable enough.
Due to the poor function of your knee before the operation, your muscles have likely weakened over several months or even years. Therefore, they will need time to regain their strength and flexibility. It is not uncommon for the knee to remain sensitive and easily fatigued during prolonged efforts or squatting.
This should not discourage you.
The time for healing, for your skeleton to adapt to your prosthesis, and for the recovery of your flexibility and strength is long. Progress will be steady, and it often takes nearly a year to achieve a “forgotten knee.”
To get there more surely and more quickly, you will be asked to do very regular sessions of knee mobilization in flexion/extension yourself, from the day after your surgery, wherever you are, in bed, sitting on your sofa, or outside, without forcing through pain.
You should not rely solely on the time spent with the physiotherapist. You remain the main actor in your recovery.






