Knee
The menisci are two crescent-shaped structures interposed between the femur and the tibia, serving both as stabilizers and shock absorbers for the knee joint.
Thus, they protect the cartilage from excessive pressure and hence wear. They have a fairly hard elastic consistency, like rubber.
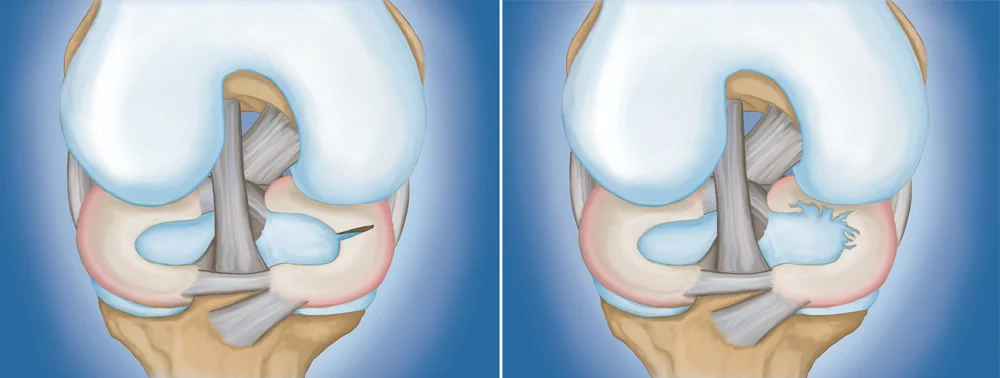
The menisci can either crack or tear following a trauma or wear down gradually over time. In both cases, a more or less significant fragment can detach and sometimes become lodged between the femur and the tibia.
ACUTE TRAUMATIC OR DEGENERATIVE LESION?
In young patients, meniscal lesions generally occur suddenly. It is often due to a pivoting movement, quickly standing up from a squatting or sitting position, a sudden acceleration/deceleration, lifting a very heavy object, landing from a jump, etc.
A sharp pain is felt, sometimes accompanied by a locking with the inability to extend and/or bend the knee completely. A more or less abundant effusion can follow within a few minutes to a few days. Degenerative meniscal lesions, on the other hand, are rather the result of progressive wear of the meniscal tissue over several months or years, with excessive mechanical stresses repeated over time.
We most often encounter them in patients over 40 years old who have quite physical sports and/or professional activities: Footballers, hikers, bricklayers, nursery assistants, etc. Certain factors can promote this meniscal degeneration, such as genu varum (“Lucky Luke” knees) and being overweight. The pains are quite chronic, fluctuating, progressively setting in, and accompanied by also fluctuating effusion.
It involves the medial meniscus in the majority of cases.
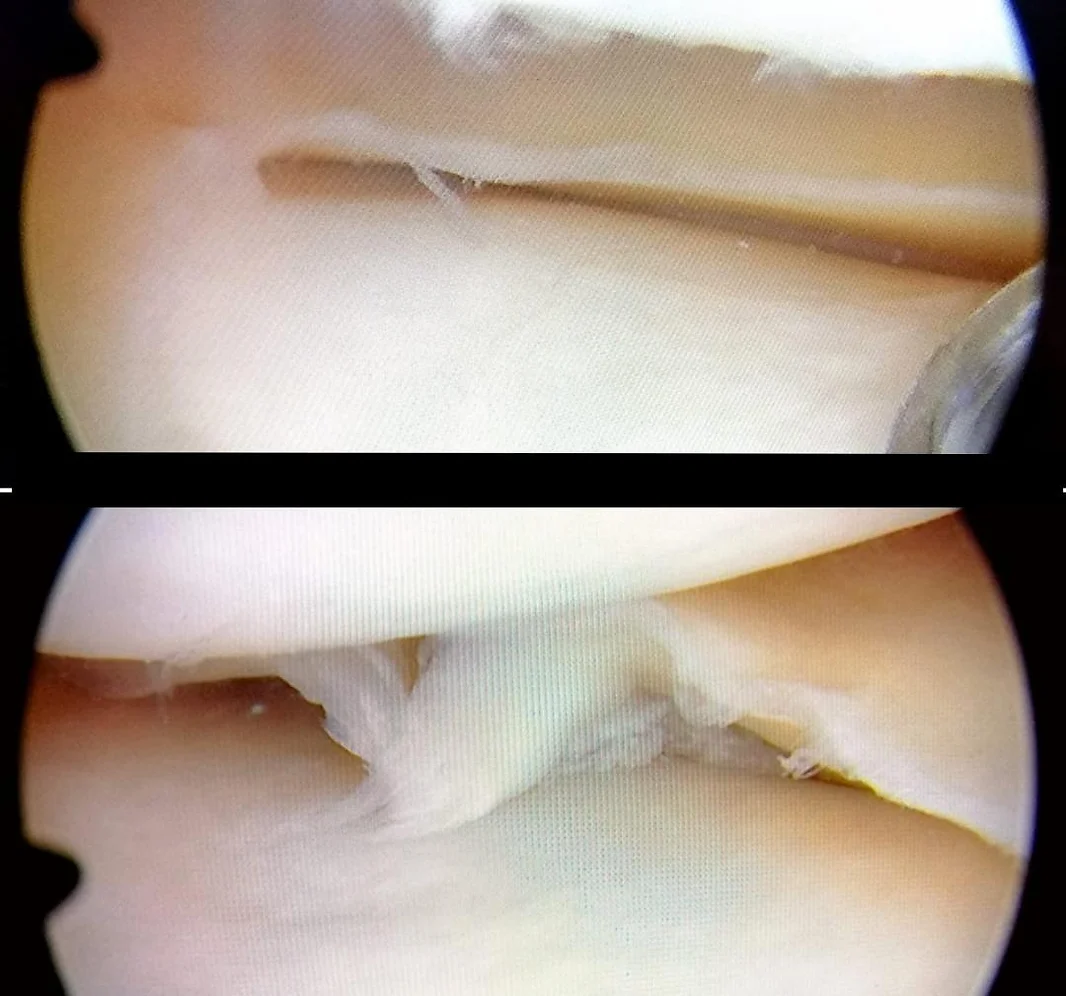
The typical image on MRI is a “horizontal tearing” of the meniscus, sometimes accompanied by small meniscal cysts. This can constitute the warning signs of arthritis of the joint.
PRINCIPLES OF TREATMENT:
While surgical resection of the entire damaged meniscus may relieve symptoms quickly and for several months, it would significantly increase the risks of osteoarthritic degeneration of the knee. We are therefore currently aiming to preserve the meniscus as much as possible. We first opt for a meniscal suture whenever the chances of healing are good.
When it comes to a non-suturable tear (significant damage, old rupture, lesion in a non-vascularized zone, etc.), we perform a meticulous excision of the damaged part only (partial meniscectomy).
In the case of a “degenerative horizontal tear,” non-surgical treatment is prioritized, since the wear generally affects the entire meniscus: Joint hygiene measures, physiotherapy, crutches, hyaluronic acid injections, PRP injections, etc.
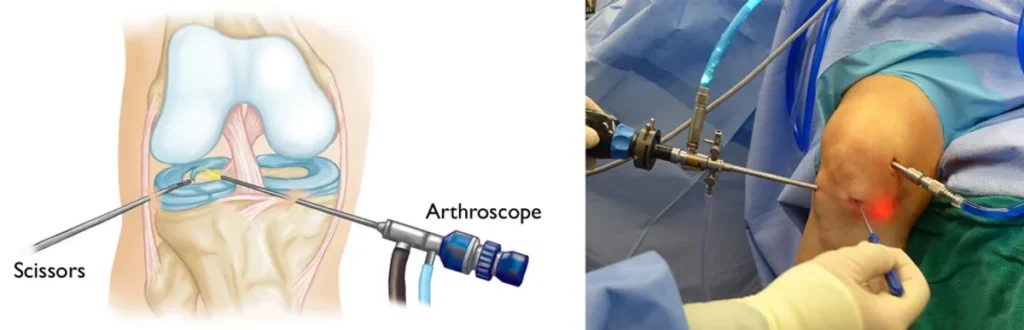
THE SURGERY:
In the vast majority of cases, the surgery is performed by arthroscopy: through two skin punctures of less than one cm, a camera (the arthroscope) and 4mm instruments are inserted into the knee to perform the surgical procedure.
The surgery is most often carried out on an outpatient basis.
Depending on your preferences and especially your medical history, the surgery is done under general anesthesia or spinal anesthesia.
Skin closure is performed using 2 sutures.
POSTOPERATIVE FOLLOW-UP:
You leave the same evening of the surgery with a dressing, a knee brace, and crutches. If it is a meniscal suture, you are not allowed to bear weight on the operated side for 6 weeks, the time necessary for the healing of the sutured meniscal lesion.
If it is a meniscectomy, you can bear weight normally from the first day. Crutches are then kept only for a few days, the time it takes to resume normal walking. In all cases, you will need to rest your knee for the 3 months following the surgery, avoiding mechanically demanding activities.
Physiotherapy sessions may be prescribed depending on the case to maintain your muscles and recover joint flexibility.
Thanks to arthroscopy and the outpatient mode, complications from meniscal surgeries have become even rarer (in the order of less than 1 case per 1,000). In case of healing failure after meniscal suture (about 20% of cases), a second surgery may be necessary to remove the part that has not healed.