Hip
Total hip replacement or THR is one of the most commonly performed surgeries in France, with about 130,000 primary procedures performed each year.
The two main indications for such surgery are displaced femoral neck fractures and hip osteoarthritis (coxarthrosis), which generally occurs after the age of 60.
In younger patients, several other pathologies can lead to such surgery: dysplasia, rheumatoid arthritis, avascular necrosis, advanced femoroacetabular impingement, etc.
In the case of hip osteoarthritis, the eroded and dried-out cartilage can no longer ensure frictionless sliding of the joint surfaces. The contact of the bare bones during joint movement becomes increasingly painful and stiffening.
DEFINITION OF A THR:
Joint replacement with a prosthesis involves the excision of damaged joint surfaces and the installation of new, smooth, and painless artificial surfaces, accurately replicating the morphology and mobility of a native hip.
Preparation for the surgery:
Preparation of the general medical condition is essential before the surgery, including:
- A cardiological assessment: Your cardiologist must evaluate your cardiac condition and certify the absence of contraindications to surgery.
- A dental check-up: Your dentist must certify the absence of a dental infection.
- If you are diabetic, your diabetes must be well-controlled. Poorly managed diabetes increases the risk of infection and healing problems.
- Verification of the absence of latent infection in your body, notably urinary tract infection.
- A general blood test.
This will be followed by a consultation with the anesthesiologist, who will analyze all these elements and propose the type of anesthesia according to your needs: General anesthesia (you are completely asleep throughout the surgery) or spinal anesthesia (injection in the back similar to an epidural, only the lower body is anesthetized). Each anesthesia method has its advantages.
If you prefer not to see, hear, or feel anything, general anesthesia is ideal for you. If you are apprehensive about falling asleep and prefer to maintain a sense of “control” over the situation, you can request spinal anesthesia. Hip replacement cannot be performed under pure local anesthesia.
Surgical planning:
We perform a digital planning or use templates for the prosthesis beforehand. This involves determining in advance the sizes and shapes of implants that match the patient’s anatomy and allowing for a faithful reproduction of the movements and anatomy of the native joint (range of motion, length of the lower limb, appropriate tension of tissues, especially the muscular sling of the gluteals).
In cases where the femoral or acetabular anatomy is unusual, it is necessary to perform a 3D planning of the prosthesis.
Moreover, we have the possibility to simulate the range of motion of the planned prosthesis, and to adjust precisely the position of each implant in the three planes of space to optimize this range to the maximum and avoid potential mechanical conflicts. 3D printing has also been helpful in planning certain difficult cases of hip dysplasia or revision THR.
The surgery:
The surgery typically lasts one hour. This duration can vary depending on the complexity of the case.
You are laid on your back on a specialized table that allows for the mobilization of the operated hip in all planes of space.
The surgical approach:
Several surgical approaches are available for performing a Total Hip Replacement (THR). Statistically, the most commonly used approach in France is the posterior approach (Moore’s approach), which requires cutting through the gluteus maximus muscle and some of the pelvitrochanteric muscles to access the joint. It provides easy access to the joint and allows for extension to the femoral diaphysis if needed, but it has a slightly higher dislocation rate and a slightly longer functional recovery than other approaches.
We have chosen to use Moore’s posterior approach only for difficult prosthesis changes (difficult THR revisions) and situations where a mini-invasive anterior approach would be contraindicated. Indeed, we perform the majority of our hip prostheses through a mini-invasive anterior approach.
This approach was described by the German C. Hueter and then developed by R. Judet, M. Siguier, and E. Letournel in France (three pioneers of orthopedic surgery in the world). It allows access to the hip without cutting through muscles. The skin incision is on average 10cm and is located at the front of the proximal thigh.
For such surgery, this is considered a small incision. But what truly makes the anterior approach “mini-invasive” is the preservation of deep structures, especially the muscles. At each depth level, muscles are successively pushed aside to reach the anterior face of the hip joint.
Once the joint procedure is completed and the prosthesis placed, the retractors are removed, and the muscles naturally return to their anatomical position. There is no need for muscle suturing.
Postoperative follow-up:
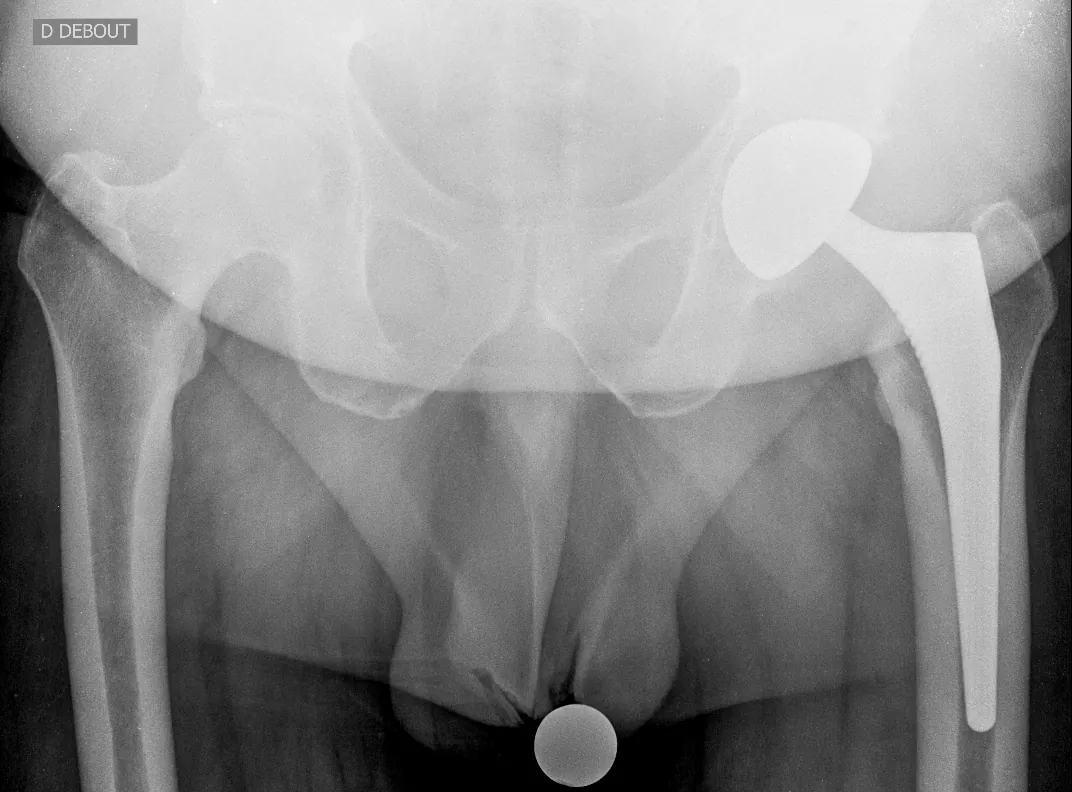
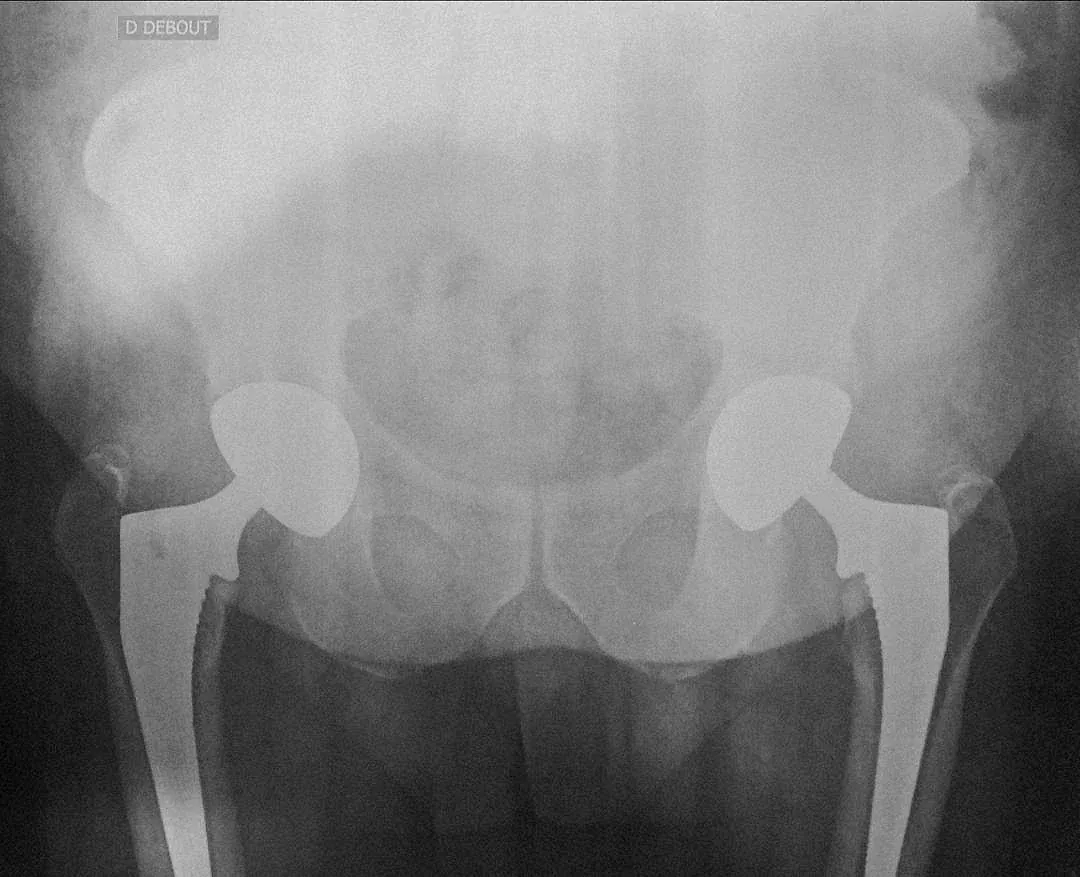
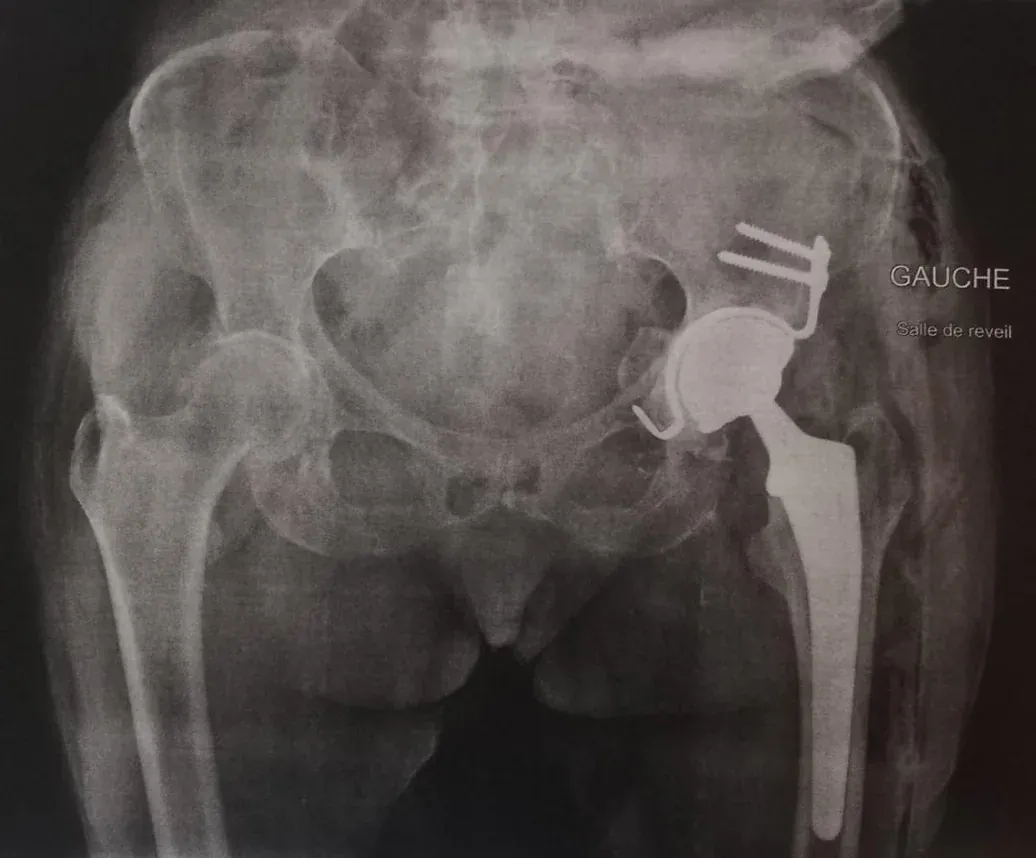
Once the surgery is completed, you are transferred to the recovery room, where you gradually wake up from the anesthesia under the watchful eyes of the nursing staff. A control X-ray is systematically requested and shown to the surgeon to verify the position of the implants once again.
You stay in the recovery room for an average of one to three hours, then a porter takes you back to your room. I visit you with the nurses at the end of the day to give you post-operative instructions, but also to help you walk.
The quick and relatively painless recovery is one of the main advantages of the mini-invasive anterior approach, and the majority of our patients manage to stand up and take a few steps in the corridor on the evening of the surgery. Even though they are allowed full weight-bearing on both legs, I strongly recommend my patients walk with two crutches for at least two weeks. This serves as protection against false movements and slips while they regain perfect control of all movements.
The next morning, a physiotherapist visits you. They help you walk, teach you how to use crutches, and have you practice a few stair steps. If you are comfortable enough walking and your control blood test is good, discharge can be authorized. The majority of our patients manage to return home the day after the surgery. Post-operative pain is generally well controlled by the prescribed medication and significantly diminishes starting from the 2nd week.
A daily injection of anticoagulants for 4 to 6 weeks reduces the risk of post-operative thrombophlebitis. Rehabilitation during the first two months following a THR is quite straightforward: You should walk, at your own pace, gradually increasing the distance and frequency each day, to gradually get your muscles, which have suffered for years from arthritic disease, back in shape.
If needed, exercises and rehabilitation sessions will follow with a physiotherapist, beyond the first two months.

Here is a photo of a scar from an anterior approach, it averages 10cm in length.

