Hip
The femoral neck fracture is one of the most common fractures in trauma surgery. Each year, most often due to a simple fall, more than 80,000 people, a majority of whom are women over 70 years old, fall victim to it. The treatment for these fractures is surgical in almost all cases.
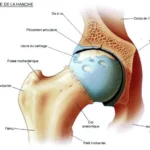
The femur forms the skeleton of the thigh; its upper end, the femoral head, which is spherical in shape, articulates with the pelvis. It is connected to the body of the femur, the diaphysis, by the femoral neck. This neck is shaped like a very strong flying buttress but works in cantilever and bears the entire weight of the body while standing, walking, and in all acts performed while bearing weight on the lower limb.
The risk of fracture increases with age:
The femoral neck fracture can affect adults of any age following a violent accident (scooter, motorcycle, car, sports, etc.), or at lower velocity among the elderly (20 to 30 times more than in young adults).
Indeed, the femoral neck, like other parts of the skeleton, becomes more fragile with age due to decreased bone density. In severe cases, this is referred to as osteoporosis. This is exacerbated by sedentary lifestyle or certain treatments (e.g., long-term high-dose cortisone), and affects women twice as much after menopause as it does men.
In the elderly, the risk of falling and therefore of fracture can be increased by a multitude of medical and non-medical factors:
- Visual disorders (AMD, loss of visual acuity, etc.)
- Balance disorders (inner ear problems, vertigo, etc.)
- Loss of muscle strength (sarcopenia)
- Neurological disorders (consequences of stroke, tumors, etc.)
- Certain medications (opioid derivatives, tranquilizers, antihypertensives, etc.)
- Insufficient fall prevention: wet floors, poorly lit rooms, carpet edges, etc.
Two types of fractures:
There are two main types of femoral neck fractures according to their location:
➜ “True cervical” fractures that affect the neck itself (1/3 of fractures)

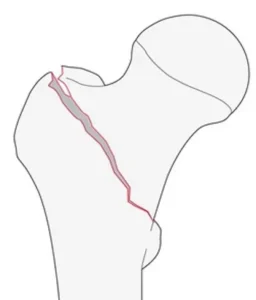
➜ Pertrochanteric fractures (2/3 of femoral neck fractures) located at the junction between the neck and the diaphysis.

An emergency situation:
In most cases, the patient has total functional impotence: they are unable to get up or walk. They experience very severe pain at the hip level (groin fold, buttocks). Most often, there is a shortening and external rotation of the lower limb.
Emergency hospitalization is necessary to confirm the diagnosis with radiographs, sometimes a CT scan if needed.
In the case of some true cervical fractures where the neck is embedded in the femoral head without detaching, the pain is less, which can be misleading. Therefore, in the slightest suspicion of a femoral neck fracture, the patient is immobilized in principle, until a precise radiological diagnosis is obtained, to avoid worsening an initially good prognosis fracture.
Two types of surgery:
Surgery is almost always performed after a femoral neck fracture, except in cases of major contraindications in some patients whose health is very deteriorated (less than 1 case out of 100).
The surgery must be carried out very quickly after the accident to give the patient the best chances of recovery and to limit the medical risks associated with prolonged bed rest (urinary infection, pneumonia, bedsores, etc.).
Displaced true cervical fractures
Pertrochanteric fractures
➜ In displaced true cervical fractures, the microvessels supplying blood to the femoral head have likely been ruptured at the time of the fracture. The risks of necrosis of the head (death of bone cells) or non-union (called pseudarthrosis) are significant.
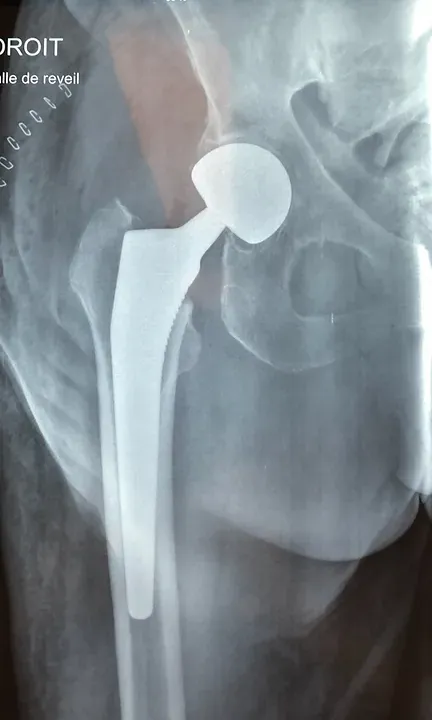
In elderly subjects, we prefer to solve the problem once and for all, and therefore often opt for prosthetic replacement of the joint (intermediate or total hip prosthesis).
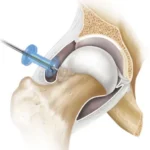
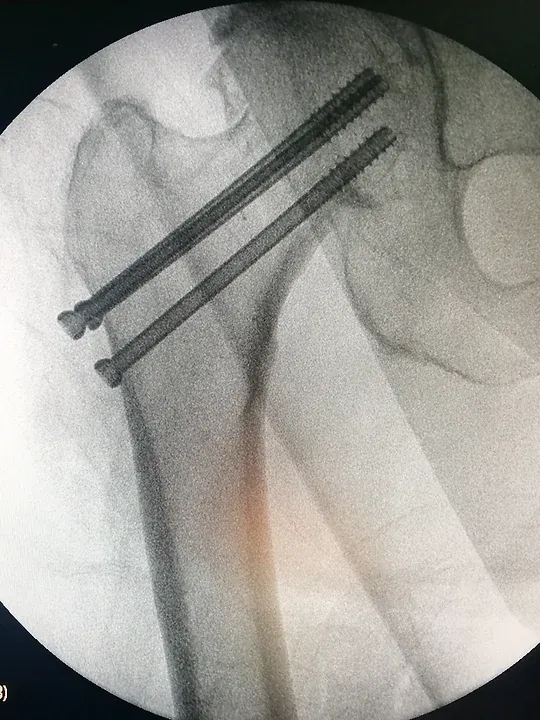
In the specific case of very young patients or in cases of non-displaced true cervical fractures, osteosynthesis with percutaneous screws or intramedullary nailing is worth attempting, in the hope of sufficient restoration of blood supply and thus a "revitalization" of the native femoral head after the fracture.
➜ In pertrochanteric fractures, the microvessels ensuring blood supply to the femoral head have probably not been affected by the fracture. The fracture is distant from their anatomical emergence point.
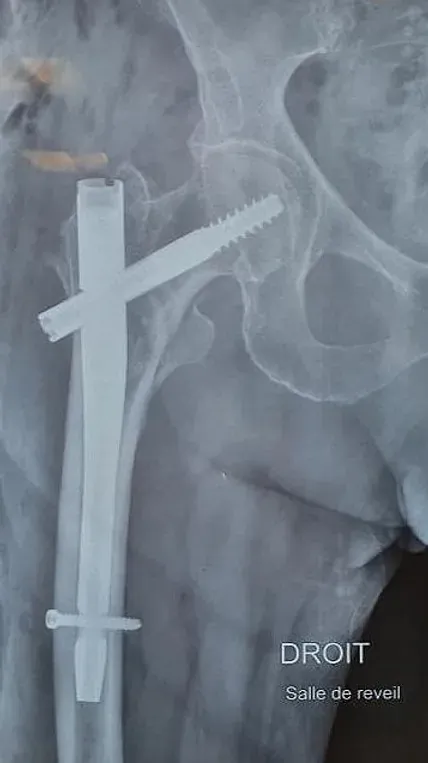
Therefore, these fractures are most often reduced and stabilized by osteosynthesis (intramedullary nail or screw-plate).
Displaced true cervical fractures
Pertrochanteric fractures
➜ In displaced true cervical fractures, the microvessels irrigating the femoral head have likely been ruptured at the time of the fracture. The risks of head necrosis (death of bone cells) or non-union (called pseudarthrosis) are significant.
In elderly subjects, we prefer to solve the problem once and for all, and therefore often opt for prosthetic replacement of the joint (either a hemiarthroplasty or total hip prosthesis).
In the specific case of very young patients or in cases of non-displaced true cervical fractures, osteosynthesis with percutaneous screws or an intramedullary nail is worth attempting, in the hope of sufficient restoration of blood supply and thus a "revitalization" of the native femoral head after the fracture.
➜ In pertrochanteric fractures, the microvessels ensuring the blood supply to the femoral head have probably not been affected by the fracture. The fracture is distant from their anatomical emergence point.
Therefore, these fractures are most often reduced and stabilized by osteosynthesis (intramedullary nail or screw-plate).

The primary goal of surgery in elderly patients is to enable them to stand and walk as soon as possible with full support.
Early complications: (surgical site infection, pulmonary embolism, etc.) are rare but can be serious.
Late complications: nonunion (lack of fracture healing), avascular necrosis of the femoral head, and prosthesis loosening often require re-intervention.
The most serious complication of femoral neck fractures in old age is the progressive post-operative deterioration of the general condition with decompensation of preexisting diseases.
In rare cases where the patient cannot undergo surgery for medical reasons, a non-surgical treatment can be performed (continuous traction of the fractured limb until consolidation) but the complications related to bed rest in an already very fragile patient are often very serious.
After the surgery:
Rehabilitation is essential after the surgery. Its duration varies according to the patient’s age and their ability to recover. It starts the day after the operation in the orthopedic and trauma surgery department and primarily consists of getting the patient to walk and gently maintaining their joint mobility.
Rehabilitation is often lengthy for elderly patients who must not only relearn to walk but also regain their independence in daily life activities (sitting, lying down, getting out of bed, bathing, etc.). Hence, the need for appropriate care after the hospital stay: either by a physiotherapist at home in the best cases, or more often, in a convalescence center or a functional rehabilitation service.
Bone consolidation of the fracture is generally achieved within six to eight weeks, justifying prolonged use of canes. In the case of a prosthesis, the hip can be immediately loaded, allowing for a quicker recovery.
Ultimately, the patient will be able to walk again, preferably with a walker (or crutches) to avoid another fall.
It’s important to know that even in the absence of complications, a femoral neck fracture often results in some partial loss of independence in elderly patients.
After 80-85 years, and for patients living alone, the femoral neck fracture is one of the most frequent reasons for admission into a nursing home.
On the other hand, a young adult, quickly autonomous with their crutches, will return home after a short hospital stay and will regain their functional abilities once the fracture has consolidated.
Here are some prevention tips:
In addition to adapting one’s home to eliminate objects on the floor that could cause a fall, the first piece of advice is to stay active. It is strongly recommended to walk every day, which helps to strengthen bone density and maintain good muscle quality.
For the same reason, it is important to have a good nutritional balance with sufficient intake of proteins and calcium. After menopause, women should also monitor their bone mineralization with exams and, in case of mineral deficiency, take appropriate supplementation.
To learn more about the care of elderly patients suffering from a hip fracture, you can consult the article published by the Haute Autorité de Santé by clicking on the following link:
Adapted from the information sheet of SOFCOT (French Society of Orthopedic and Traumatological Surgery)